
There are a few gynaecological surgeries that can lead to surgical menopause either automatically or as a result of compromised ovarian blood supply. Different parts of the reproductive system can be targeted for various medical reasons. The female reproductive system consists of the ovaries, uterus, cervix, vagina, and fallopian tubes. The ovaries produce eggs and hormones, the uterus is where a fertilised egg can develop into a foetus, the cervix connects the uterus to the vagina, the vagina serves as the birth canal, and the fallopian tubes transport eggs from the ovaries to the uterus.
Surgical menopause results from the removal of both ovaries, which is called a bilateral oophorectomy (BO). When the fallopian tubes are also removed, the procedure is called a bilateral salpingo-oophorectomy (BSO). Multiple scenarios can play a role, and it’s not unusual for many factors to combine, leading to the removal of the ovaries and adjacent organs. Surgery can happen in many stages (hysterectomy, unilateral oophorectomy, partial oophorectomy, etc.), but once the last ovary is removed, surgical menopause is automatically triggered.
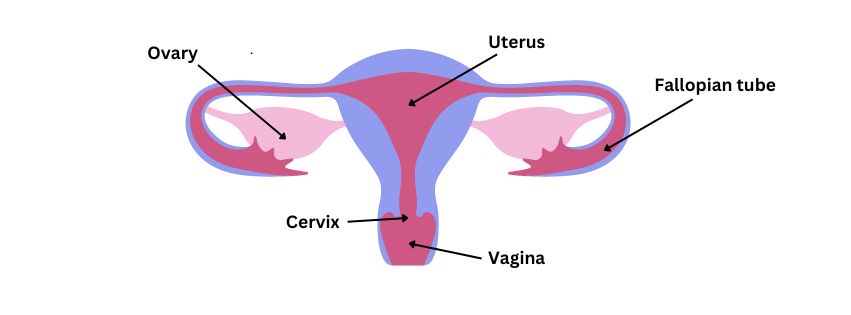
Image: Female reproductive system
The surgeries that automatically lead to surgical menopause:
- Unilateral oophorectomy (remaining ovary removed)
- Bilateral oophorectomy (BO)
- Bilateral salpingo-oophorectomy (BOS)
- Hysterectomy with unilateral (remaining ovary) or bilateral oophorectomy or salpingo-oophorectomy
The surgeries that can lead to early menopause if the ovaries are affected by the surgery:
- Radical hysterectomy (ovaries remained but are compromised)
- Unilateral oophorectomy (one ovary remained but is compromised)
- Partial oophorectomy (ovary tissue remained but is compromised)
- Total hysterectomy (ovaries remained but are compromised)
Surgeries that Automatically Lead to Surgical Menopause
Unilateral Oophorectomy (Remaining Ovary Removed)

Image: Unilateral oophorectomy (UO) (remaining ovary removed)
Definition: Surgical removal of one ovary. In the context of surgical menopause, we’re specifically referring to the removal of the remaining ovary after a previous surgery has already removed the other ovary.
Indications: Ovarian cysts or tumours; Ovarian torsion; Recurrent ovarian cancer; Severe endometriosis; Chronic pelvic pain; Completion of risk-reducing surgery for individuals who initially opted for partial risk reduction.
Impact: Immediate onset of surgical menopause if this was the only remaining ovary; Permanent infertility; Increased long-term health risks; Psychological impact due to the finality of losing reproductive function; May require adjustments to existing HRT or alternatives if already on some treatment after the first oophorectomy.
Bilateral Oophorectomy
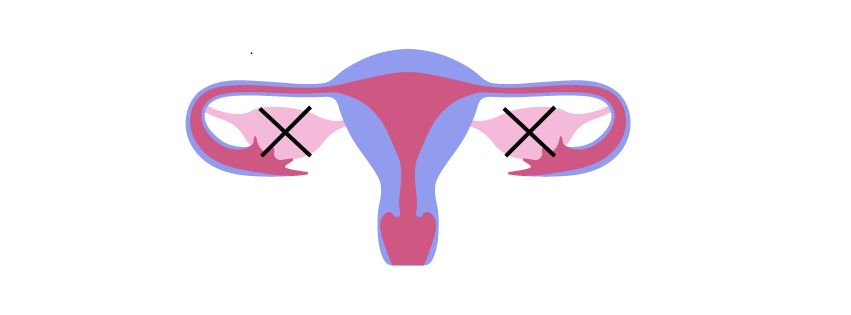
Image: Bilateral oophorectomy (BO)
Definition: Surgical removal of both ovaries.
Indications: Ovarian cancer or high risk of ovarian cancer; Severe endometriosis; Chronic pelvic pain; Ovarian torsion affecting both ovaries; Premenstrual syndrome (PMS) or premenstrual dysphoric disorder (PMDD); Polycystic ovarian syndrome (PCOS).
Impact: Immediate onset of surgical menopause; Increased long-term health risks; Requires HRT or alternatives; Psychological impact due to the finality of losing reproductive function; Permanent infertility.
Bilateral Salpingo-Oophorectomy
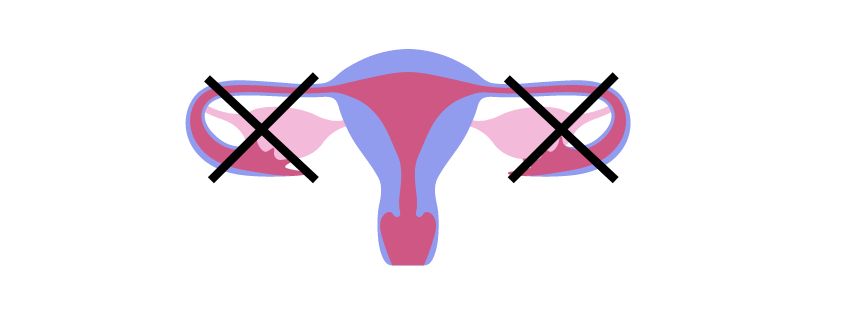
Image: Bilateral salpingo-oophorectomy (BSO)
Definition: Surgical removal of both ovaries and fallopian tubes.
Indications: Similar to oophorectomy, plus risk reduction for fallopian tube cancer.
Impact: Immediate onset of surgical menopause; Increased long-term health risks; Requires HRT or alternatives; Psychological impact due to the finality of losing reproductive function; Permanent infertility.
Prophylactic Oophorectomy (Unilateral or bilateral)
Definition: The preventive removal of one or both ovaries in the absence of cancer to reduce the risk of developing ovarian cancer. The term “prophylactic oophorectomy” refers to the removal of healthy ovaries during surgery, typically performed to achieve future benefits.
Indications: High genetic risk for ovarian cancer (e.g., BRCA1 or BRCA2 mutations); Strong family history of ovarian cancer; Lynch syndrome or other hereditary cancer syndromes; As part of risk-reducing surgery in breast cancer patients.
Impact: If bilateral, immediate onset of surgical menopause; Significant reduction in ovarian cancer risk; Reduction in breast cancer risk (if perimenopausal); Hormonal changes leading to menopausal symptoms if both ovaries are removed; Potential need for hormone replacement therapy; Psychological impact of cancer risk reduction versus immediate menopausal symptoms; Fertility implications depending on whether one or both ovaries are removed.
| Prophylactic Oophorectomy: Making a Decision The decision should be made after careful consideration of your individual risk factors, age, and personal preferences. Discussion on impacts on fertility and options for fertility preservation. The balance cancer risk reduction and quality of life considerations should be thoroughly discussed with healthcare providers. Often requires nuanced decision-making, taking into account your overall health, cancer risk, desire for future fertility, and preferences regarding menopausal symptoms and hormone replacement therapy. |
Total/Radical Hysterectomy with unilateral (remaining ovary) or bilateral oophorectomy (or salpingo-oophorectomy)
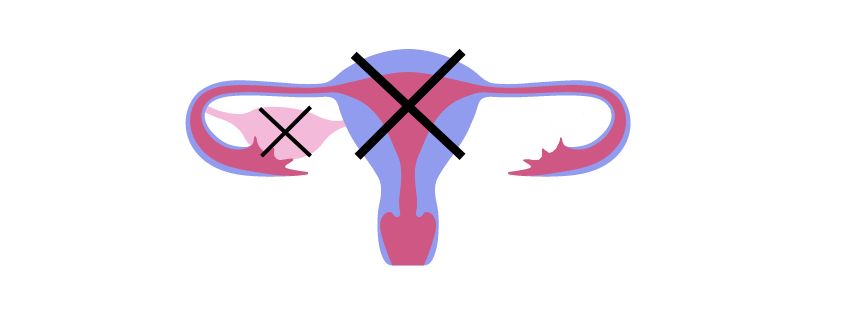
Image: Total hysterectomy with unilateral oophorectomy (THUO) (remaining ovary)
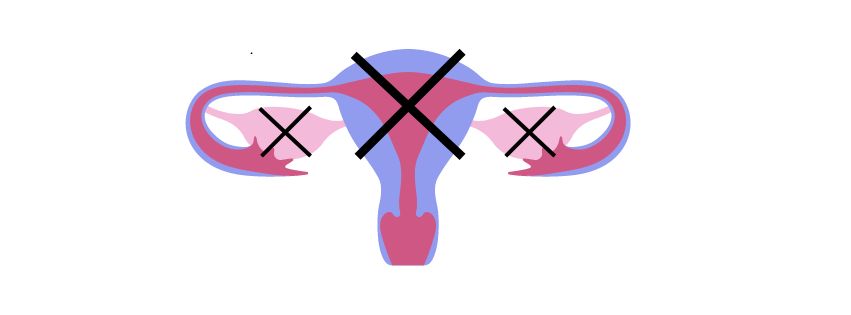
Image: Total hysterectomy with bilateral oophorectomy (THBO)
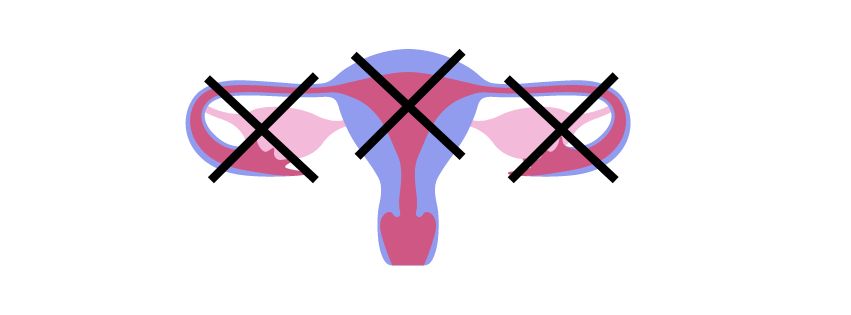
Image: Total hysterectomy with bilateral salpingo-oophorectomy (THSBO)
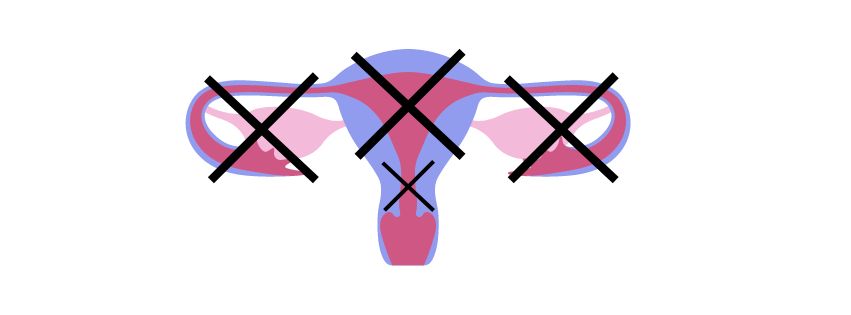
Image: Radical hysterectomy with bilateral salpingo-oophorectomy (RHBSO)
Definition: Surgical removal of the uterus with one or both ovaries or one or both ovaries and fallopian tubes.
Indications: In addition to the indications mentioned for bilateral oophorectomy, a hysterectomy may be indicated for the following reasons: Uterine fibroids; Severe endometriosis (with or without adenomyosis); Uterine prolapse; Heavy menstrual bleeding (menorrhagia) that has not responded to other treatments; Enlarged uterus pressing on other organs; Chronic pelvic pain; Invasive cancer of the uterus, cervix, vagina, fallopian tubes or ovary; Serious complication during childbirth (rupture of the uterus).
| Beware, sometimes, the ovaries are removed opportunistically but without solid medical reasons. This practice is discouraged nowadays but still in practice. Many women have been told that once postmenopausal their ovaries were not necessary and therefore encouraged to have them removed when undergoing a hysterectomy. If your surgeon recommends the removal of your ovaries, no matter your age, make sure they can justify the surgery and if they can’t, don’t hesitate to ask for a second opinion. |
Surgeries that Can Potentially Lead to Surgical Menopause or Early Menopause
Unilateral Oophorectomy (One Ovary Remained)

Image: Unilateral oophorectomy (UO)
Definition: Surgical removal of one ovary.
Indications: Ovarian cysts or tumours; Ovarian torsion; Recurrent ovarian cancer; Severe endometriosis; Chronic pelvic pain; Risk-reducing surgery.
Impact: Possible reduction in fertility; Potential surgical menopause if the remaining ovary is damaged; Possible irregular menstrual cycles or earlier onset of natural menopause; Potential increased long-term health risks if the remaining ovary is damaged; May require HRT or alternatives.
Partial Oophorectomy
Definition: Surgical removal of part of an ovary, leaving some ovarian tissue intact.
Indications: Benign ovarian cysts or tumours; Endometriosis affecting part of the ovary; Ovarian torsion with partial ovarian preservation; Fertility preservation in cases requiring some ovarian tissue removal.
Impact: Potential preservation of some ovarian function and hormone production; Possible reduction in fertility, depending on the amount of ovarian tissue remaining; Potential surgical menopause if the remaining ovary is damaged; Potential need for further surgery if pathology returns in remaining tissue; Regular monitoring of the remaining ovarian tissue (cancer scenario); Possible irregular menstrual cycles or earlier onset of natural menopause; Less impact on long-term health compared to complete oophorectomy; Psychological benefit of retaining some natural ovarian function.
Total Hysterectomy (Ovaries Remained but are Compromised)
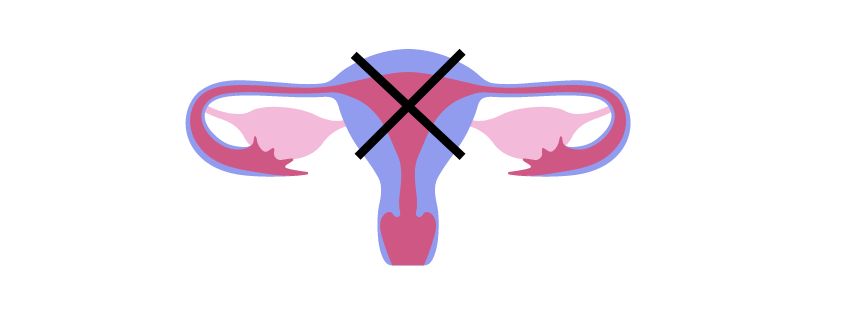
Image: Total hysterectomy (TH)
Definition: Surgical removal of the uterus and cervix.
Indications: Uterine fibroids, severe endometriosis, uterine prolapse, abnormal uterine bleeding, chronic pelvic pain, gynaecological cancers.
Impacts: Cessation of menstrual periods, inability to become pregnant, potential for earlier onset of natural menopause and possible changes in sexual function or sensation.
Radical Hysterectomy (Ovaries Remained but are Compromised)

Image: Radical hysterectomy (RH)
Definition: Surgical removal of the uterus, cervix, upper part of the vagina, and surrounding tissues (associated pelvic ligaments and lymph nodes).
Indications: Cervical cancer, advanced uterine cancer, some cases of recurrent pelvic cancer.
Impacts: All impacts of total hysterectomy, potential impact on bladder and bowel function, more extensive recovery period, possible impact on sexual function due to vaginal shortening.
| For all these procedures, it’s important to note: The psychological impact can be significant, affecting body image and sense of femininity. Recovery times and experiences vary based on the individual and the surgical approach used. Long-term follow-up care is crucial, especially for managing menopausal symptoms and associated health risks. The decision for following treatments should be made on an individual basis, considering your overall health, cancer risks, and personal preferences. |
References
Lawson AA, Rentea RM. Oophorectomy. StatPearls. Treasure Island (FL): StatPearls Publishing; Jan 2022, [Updated: 8 May 2022].
Ward, SM, Scioscia, EA. Salpingo-Oophorectomy. Medscape. [Updated: 26 Aug 2021].
Cleveland Clinic, Oophorectomy. [Updated: 12 Sept 2022].
Mayo Clinic, Oophorectomy (ovary removal surgery). [Created: 17 April 2024].
Cleveland Clinic, Hysterectomy. [Updated: 31 May 2024].
Webmd, Oophorectomy. [Reviewed: 2 March 2023].
[Updated: 17 Sept 2024]
