
Introduction: Surgical Menopause in New Zealand & Around the World
What is Surgical Menopause?
Surgical menopause occurs when a woman’s ovaries are removed before reaching natural menopause, either as part of a hysterectomy or through a bilateral oophorectomy (removal of both ovaries). This procedure leads to an abrupt decrease in hormone levels – particularly estrogen, progesterone, and testosterone – causing immediate menopause. Women may undergo surgical menopause to prevent or treat conditions such as ovarian cancer, endometriosis, or chronic pelvic pain.
Globally, approximately 1 in 8 women undergo early or premature menopause before reaching natural menopause. Despite the prevalence, there remains a lack of recent data, highlighting the need for updated research and better data collection methods.
Global Trends Hysterectomy & Data Collection Challenges
Global Trends Hysterectomy
According to the World Health Organisation, around 1.54 million women worldwide underwent hysterectomies in 2016. This surgery is commonly performed on women between the ages of 40 and 45, with about 37–39% of women having had the procedure by the age of 65.
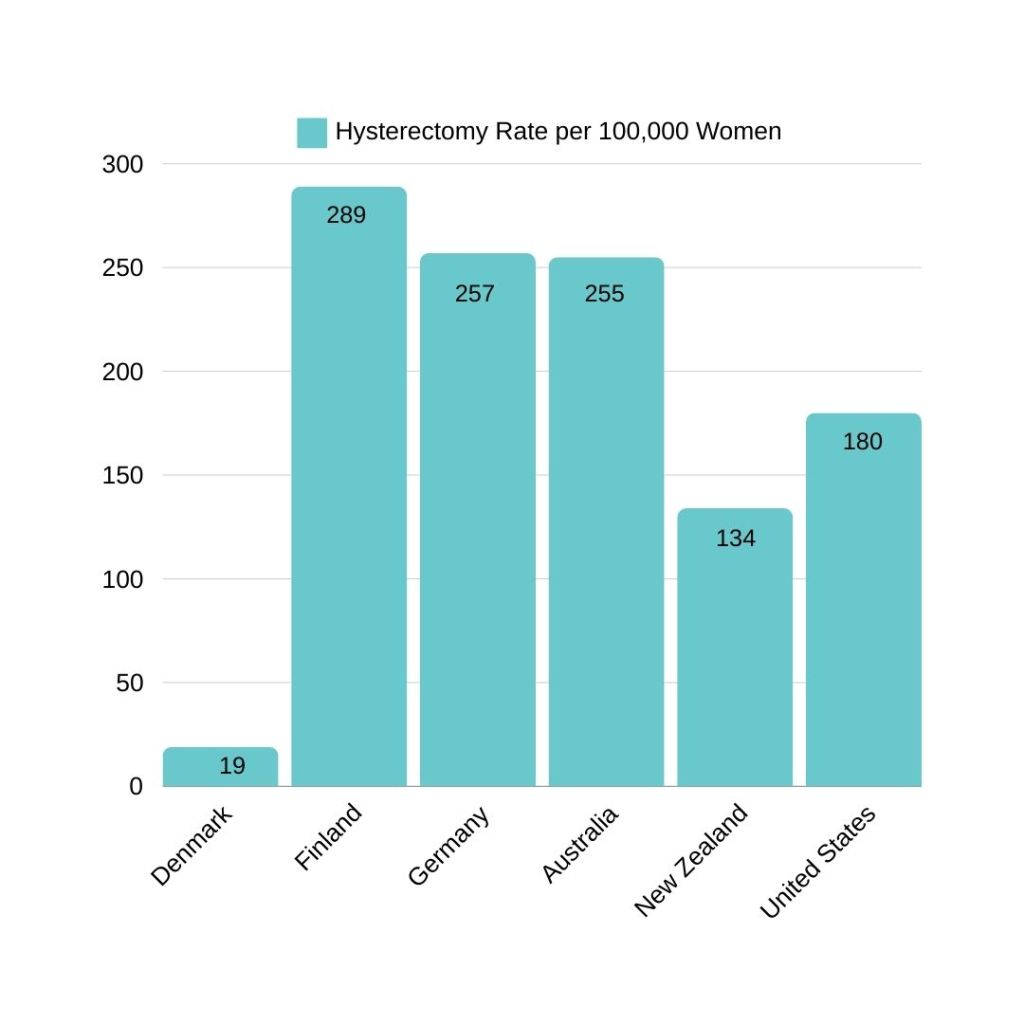
Hysterectomy rates vary widely depending on cultural, healthcare system, and policy differences:
| Country | Rate per 100,000 women | Approximate ratio |
| Denmark | 19 | 1 in 5,263 |
| Finland | 289 | 1 in 346 |
| Germany | 257 | 1 in 389 |
| Australia | 255 | 1 in 392 |
| New Zealand | 134 | 1 in 746 |
| United States | 180 | 1 in 556 |
Hysterectomy is one of the most frequently performed gynaecological surgeries. In Australia, about 30% of women will undergo a hysterectomy by the age of 70, and in the United States, approximately 45% of women will have the surgery at some point in their lives.
Challenges in Accurate Data Collection
Accurately determining the number of women affected by surgical menopause is difficult due to several factors:
Data Inconsistencies & Terminology
The term “hysterectomy” may or may not include oophorectomy, and many databases do not clarify whether one or both ovaries were removed.
Multiple Surgeries & Data Duplication
A single woman may have several related surgeries, such as salpingectomy, oophorectomy, and hysterectomy, which are often recorded separately and may be double-counted.
Limited Research
Surgical menopause remains under-researched. Few studies track women before and after oophorectomy to assess long-term health impacts.
See the Self-Advocacy section for more on the gender health gap.
New Zealand Context & Data Analysis
Estimating the Number of Women Affected
Women in New Zealand face significant challenges due to surgical menopause, particularly in the areas of data accuracy and continuity of care.
Public hospital discharge data on hysterectomies spans from 1979/1980 to 2019/2020, but inconsistencies in recording due to changes in coding systems have made long-term comparisons difficult. Between 1999/2000 and 2007/2008, data clearly documented whether one or both ovaries were removed during hysterectomy. However, since 2008, these procedures have been grouped under the term “adnexa removal,” (which includes ovaries and fallopian tubes), without specifying whether the oophorectomy was bilateral.
Separate data on independent oophorectomy procedures exists from 1999/2000 to 2019/2020 but also lacks details on laterality. Private hospital data is even more limited.
Estimation Methodology
The lack of precise data limits our ability to accurately determine how many women experience surgical menopause. At best, we can estimate the number of women likely impacted by early or surgical menopause, which can be defined as the removal of at least one ovary during a surgical procedure.
To estimate the number of women affected by early or surgical menopause, we analysed data from 1999/2000 to 2018/2019. We included: hysterectomies with oophorectomy and independent oophorectomies. We focused on women under 45. For the 2008–2019 period, we assumed that “adnexa removal” continued to include removal of one or both ovaries, as in earlier years. Though this method has limitations, it provides a working estimate.
Private sector data was even less detailed. We combined available figures, acknowledging that not all procedures involved ovary removal.
Age Distribution
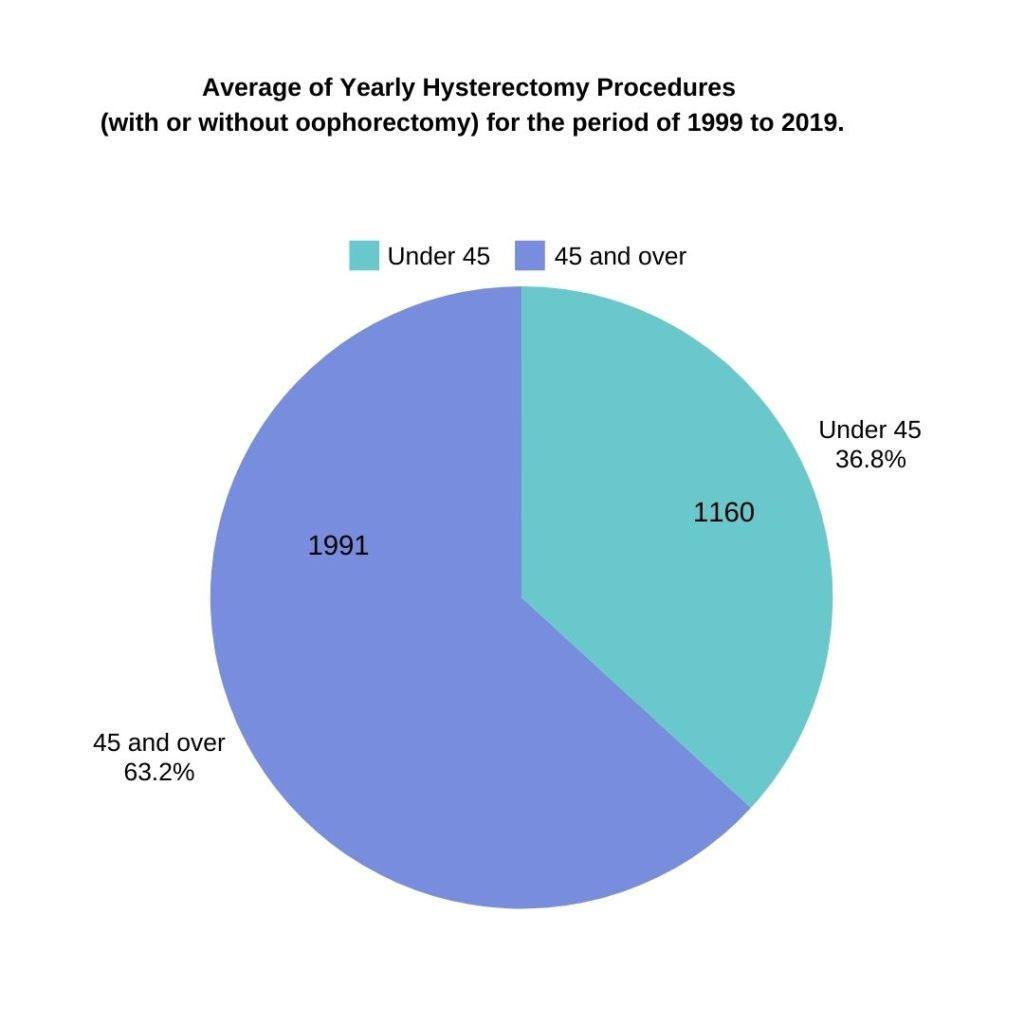
In the public sector, over a 20-year period, an average of 3,151 New Zealand women underwent hysterectomies each year (with or without ovary removal), with 37% (about 1,160 women) under the age of 45.
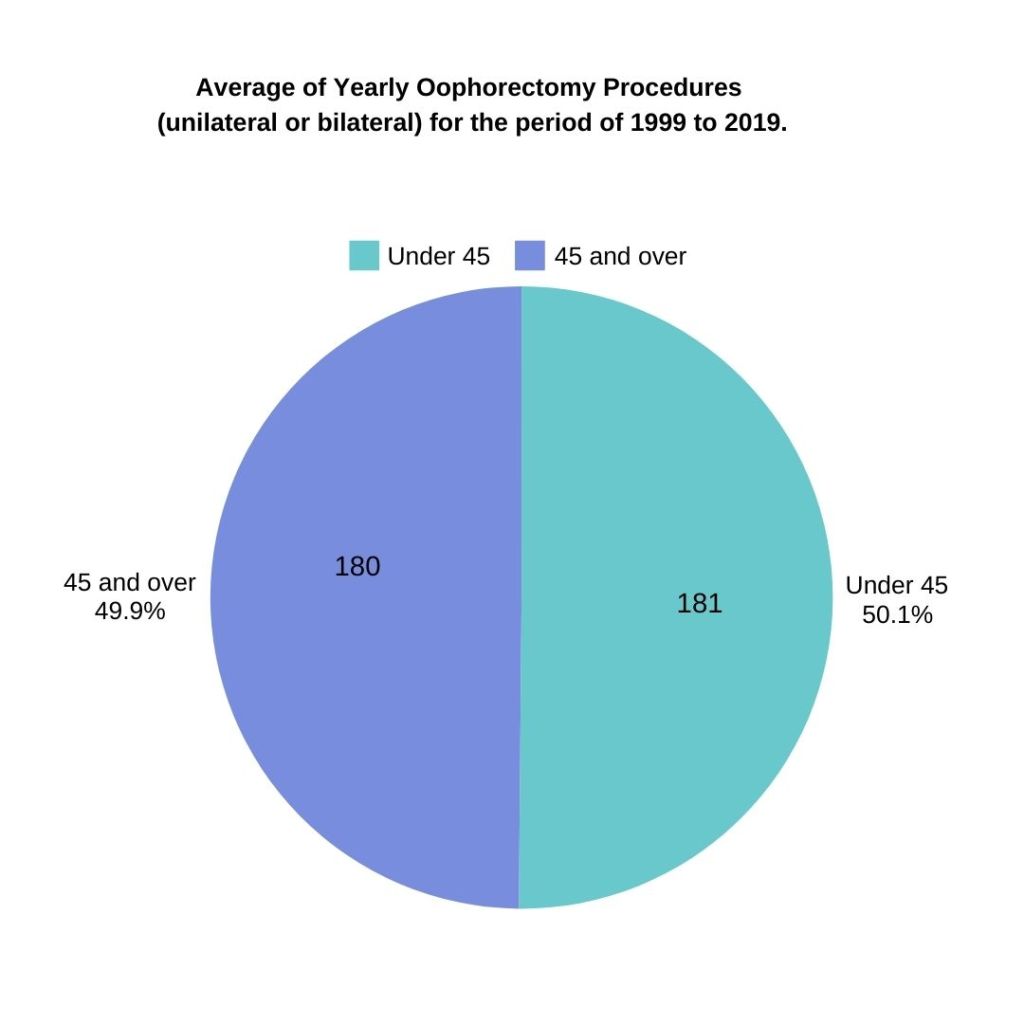
For independent oophorectomies, an average of 361 women underwent surgery annually, with 50% (around 181) under the age of 45.
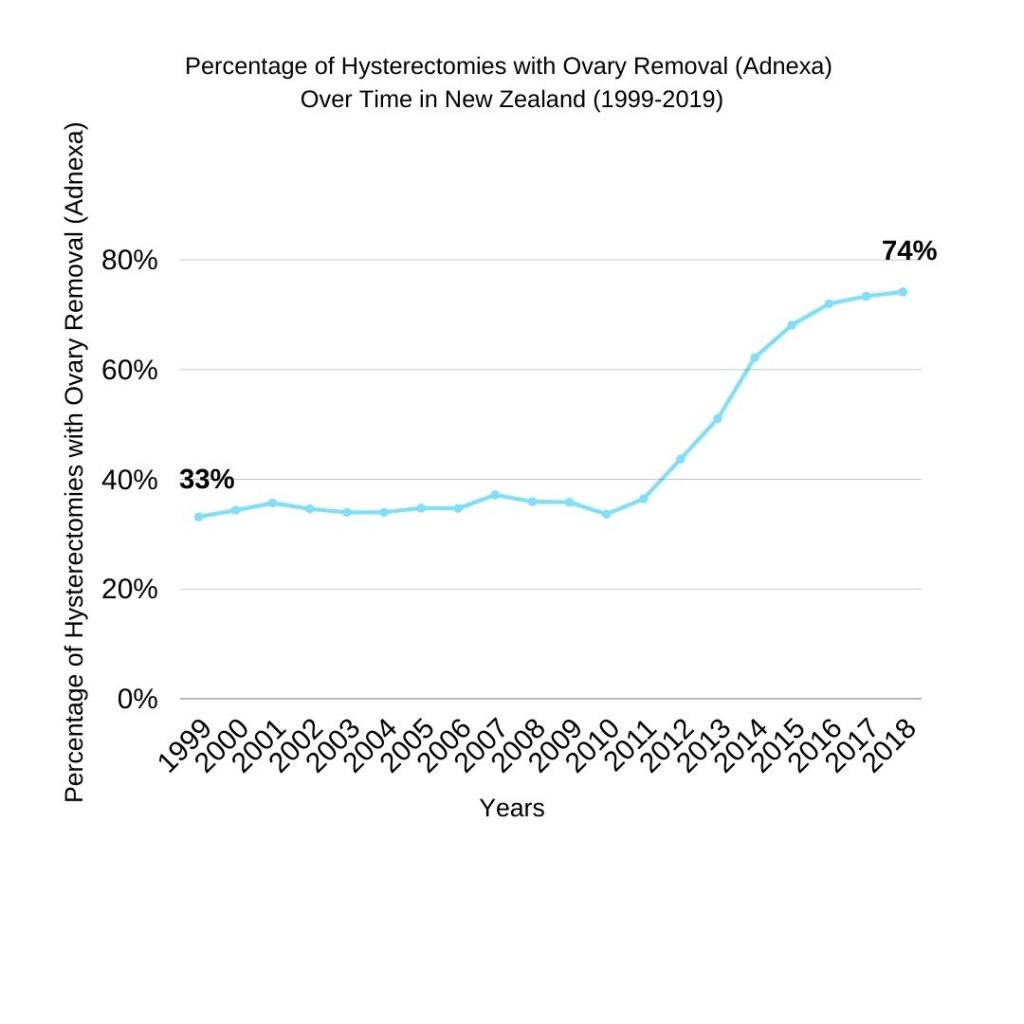
The total number of adnexa removal surgeries in the public sector increased from 33% in 1999/2000 to 74% in 2018/2019, suggesting a trend toward more comprehensive surgeries to reduce cancer risk. This shift is also likely due to advancements in surgical techniques, increased healthcare access, and a focus on preventive strategies.
In 2018/2019, within the public sector only, 884 (35%) of the 2,501 combined gynaecological surgeries—including hysterectomies with the removal of one or both ovaries (or adnexa), as well as independent oophorectomies – were performed on women under 45. Notably, more than half of all independent oophorectomies were carried out on this younger demographic, emphasising the significant impact of these surgeries on women in their reproductive years.
Trends Over Time
Over the two decades, public data indicates a significant evolution in surgical practices regarding hysterectomies in New Zealand. The total number of hysterectomies, with or without adnexa removal, has decreased from 3,423 in 1999/2000 to 2,987 in 2018/2019. Despite this decline, the proportion of hysterectomies that involve adnexa removal has risen, reflecting a more aggressive approach to cancer prevention, particularly concerning ovarian cancer, which ranks as the fifth most common cancer among women in the country and a leading cause of cancer-related deaths.
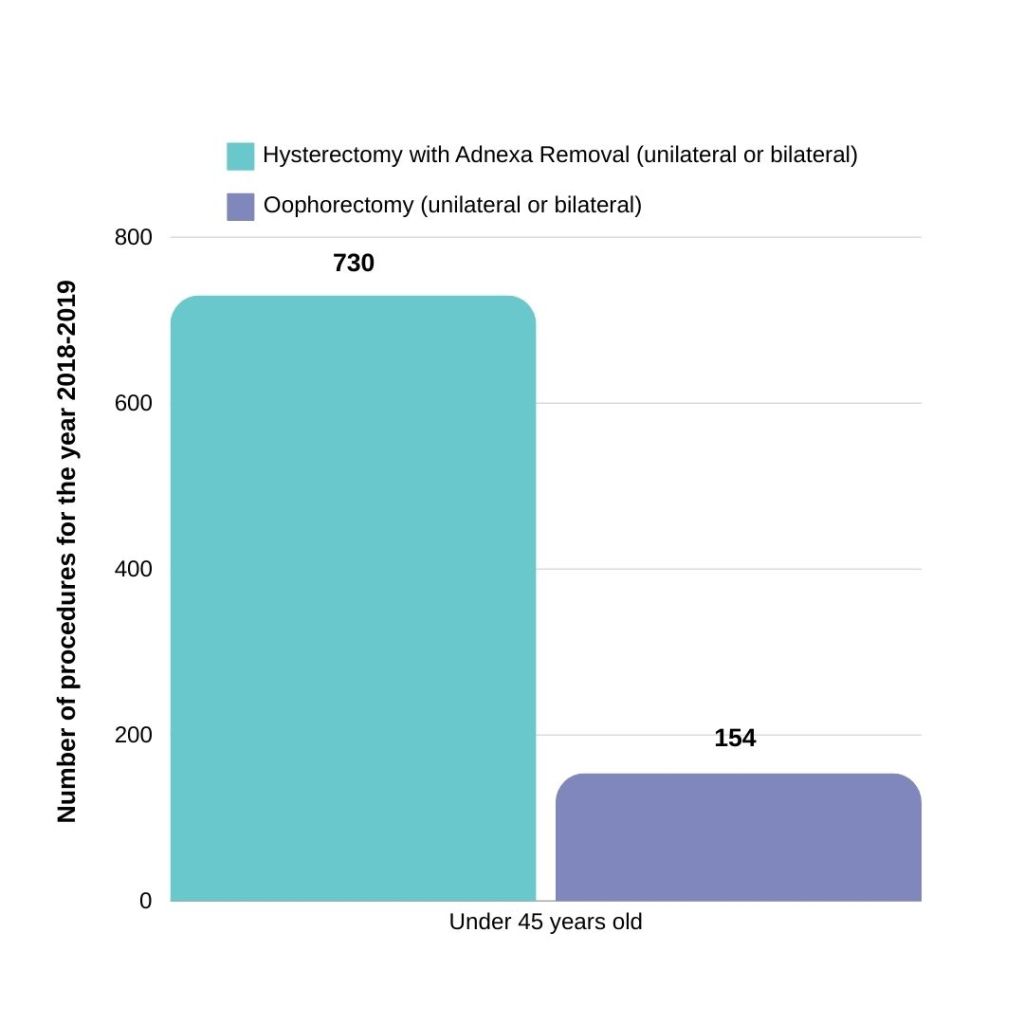
For younger women under 45, the number of adnexa removal surgeries has increased from 288 cases (25%) in 1999/2000 to 730 cases (33%) in 2018/2019. Although oophorectomy rates in this demographic have remained stable, the consistent number of younger women undergoing these procedures underscores the necessity for ongoing support and resources to manage the long-term effects of early and surgical menopause. The overall decline in hysterectomies may signal a shift toward less invasive treatments when appropriate, yet the persistence of these surgeries highlights the critical need for adequate care and management strategies for these women.
Private Sector Data & Gaps
Private sector data for 2018/2019 shows 1,784 hysterectomies, with 651 patients under the age of 45, but the specific number involving adnexa removal is unclear. Additionally, at least 416 independent oophorectomies were performed, with 111 patients under 45.
The estimated number of women who experienced early or surgical menopause, assuming all private sector hysterectomies in 2018/2019 included ovary removal, could be as high as 1,646 women under 45 across both public and private sectors, representing 1 in every 833 women in this age group. Across all age groups, up to 4,701 women – roughly 1 in 526 – may have been affected by early or surgical menopause due to ovary removal. Since early or surgical menopause result in a permanent hormonal shift, this can have profound impacts on these women’s health and quality of life, no matter their age.
Data Constraints
A sharp rise in hysterectomies occurred between 2018/2019 and 2019/2020 in the public sector, with a 363% increase in surgeries performed on women under 45.
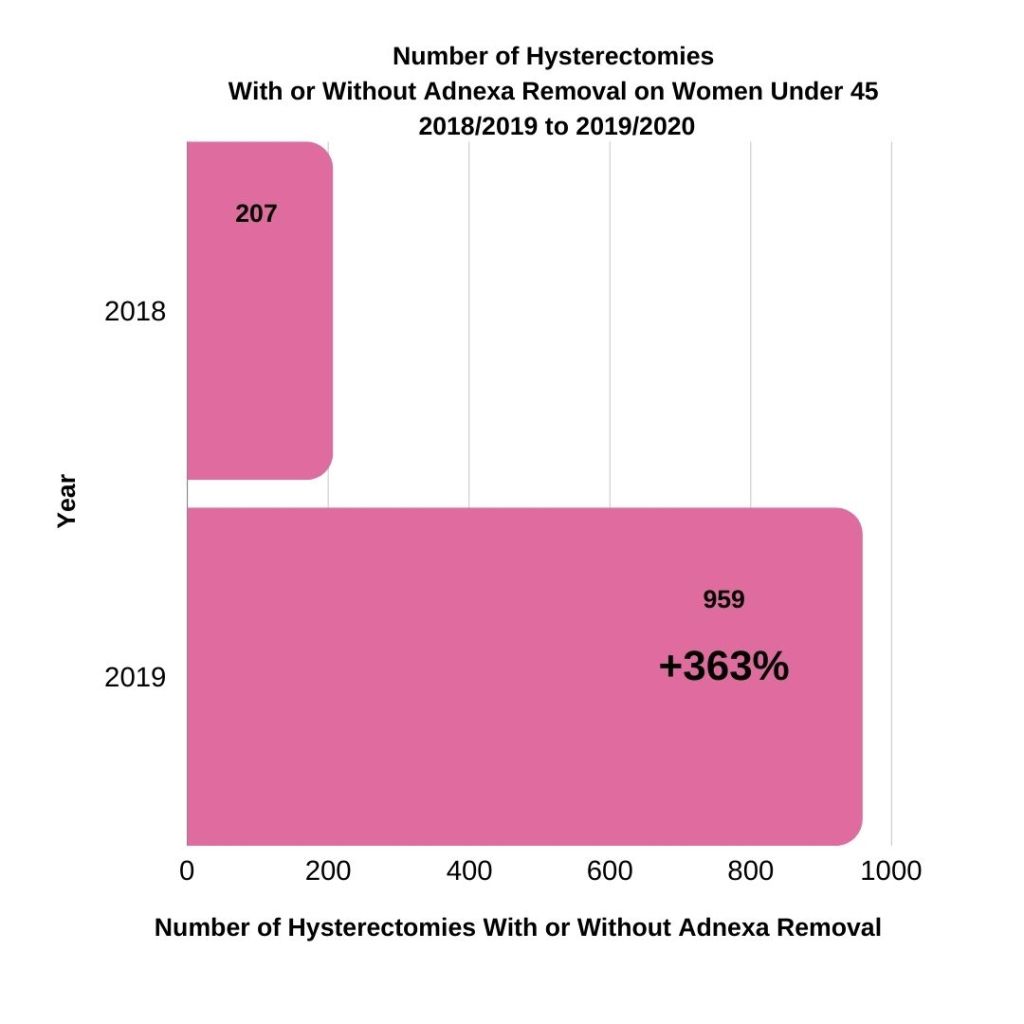
For all ages, hysterectomies with or without oophorectomy rose only by 5.2% in the public sector. The reasons behind this rise among younger women warrant further exploration.
However, the 2019/2020 public hysterectomy data did not specify whether ovaries were removed, and post-2020 data is unavailable, raising concerns about the declining quality of health records. This lack of reliable, up-to-date information hinders efforts to fully understand the scope of surgical menopause in New Zealand, making it challenging to ensure adequate care and support for women.
Health Impacts of Surgical Menopause
Surgical menopause leads to a sudden loss of hormone production, increasing the risk of:
- Osteoporosis and bone fractures
- Cardiovascular disease
- Cognitive impairment
- Sleep disturbances
- Depression and anxiety
- Sexual dysfunction
These risks require proactive, ongoing care.
Lack of Transparency & Post-Surgical Support
A 2022 nationwide survey found only 3% of women felt adequately informed before undergoing surgery that led to surgical menopause. Without full disclosure of risks and ongoing care needs, true informed consent is not possible.
It is critical that patients receive comprehensive, accessible information before and after surgery, including:
- Available treatments
- Long-term health risks
- Hormonal changes
- Symptom management
Hormone Replacement Therapy (HRT)
For women under 45, HRT is the most commonly recommended treatment following surgical menopause. It helps reduce long-term risks like osteoporosis and cardiovascular disease.
However, challenges remain:
- Many women report receiving no information about HRT pre-surgery (51% in a national survey).
- Some are advised to “see how they go,” reflecting a passive approach.
- Access to HRT is inconsistent, with Māori, Pacific, and Asian women less likely to be prescribed HRT than their European counterparts.
- Alternative treatments are needed for those who cannot or choose not to use HRT.
This gap in care is partly due to surgeons not engaging in follow-up or being unaware of the profound impact surgical menopause has on their patients’ quality of life. General lack of awareness about menopause also contributes to this inattention in doctor’s offices.
Lack of Medical Training
Medical professionals in New Zealand often lack formal training in menopause care:
- Menopause receives limited attention in medical school.
- There is no standardised postgraduate training in menopause management.
- The proportion of GPs has dropped from 40% to 25% since 2000.
This knowledge gap leaves many GPs unable to confidently support patients post-surgery, with women often left to educate themselves or seek specialised care.
As a result, women undergoing surgical menopause often face a healthcare system ill-equipped to provide the specialised care they need. This gap in knowledge can leave women without the support or guidance required to manage the complex symptoms and health risks associated with surgical menopause effectively.
Many women are left to scramble with their GPs on how to better care for themselves and unfortunately their GPs also have variable/limited knowledge of the implications of surgical menopause.
Financial & Professional Impact
Surgical menopause places a considerable financial and professional strain on women, especially those in their peak working years. Coping with severe symptoms like hot flushes, fatigue, and mood swings can hinder their productivity and ability to maintain employment.
While treatments like hormone replacement therapy (HRT) or alternative options can help alleviate some of these symptoms, they may not fully manage all the effects, leaving women to continue navigating ongoing challenges.
Additionally, healthcare costs tend to rise as women require ongoing treatment for the long-term effects of surgical menopause, such as osteoporosis or cardiovascular issues.
For more detailed information, refer to the Financial Impact section.
Recommendations to Improve Care
- Standardised Training: Introduce mandatory postgraduate menopause education for GPs and gynaecologists.
- Personalised Care Plans: Ensure every woman undergoing surgical menopause receives an individualised care plan.
- Expanded Treatment Access: Improve access to HRT and alternative therapies, particularly for underserved communities.
- Improve Data Collection: Strengthen coding and record-keeping to better track who is affected and what care they receive.
Surgical menopause is a major women’s health issue. The growing number of adnexa removal surgeries and the long-term health risks associated with surgical menopause highlight the need for better care and support systems.
References
Rout, D., Sinha, A., Palo, S.K. et al. Prevalence and determinants of hysterectomy in India. Sci Rep 13, 14569 (2023).
The NZ Menopause Survey by Menodoctor (July 2023).
Ministry of Health, Hospital Event Data and Statistics, [Accessed: Aug 2024].
Health New Zealand, Total of Hysterectomy Procedures During Publicly Funded Hospital Discharges (1979-2020).
Health New Zealand, Total of Oophorectomy Procedures During Publicly Funded Hospital Discharges (1999-2020).
Health New Zealand, Privately Funded Hospital Procedures in 2018-2019.
Medical Council of New Zealand, Informed Consent, (June 2021).
Australasian Menopause Society, Surgical Menopause [updated: Jan 2017].
Tuesley KM, Protani MM, Webb PM, Dixon-Suen SC, Wilson LF, Stewart LM, Jordan SJ. Hysterectomy with and without oophorectomy and all-cause and cause-specific mortality. Am J Obstet Gynecol. 2020 Nov;223(5):723.e1-723.e16.
European Society of Endocrinology, Large-scale Finnish study discovers link between premature menopause and mortality risk, [updated: May 2024].
Shuster LT, Gostout BS, Grossardt BR, Rocca WA. Prophylactic oophorectomy in premenopausal women and long-term health. Menopause Int. 2008 Sep;14(3):111-6.
Harvey SV, Pfeiffer RM, Landy R, Wentzensen N, Clarke MA. Trends and predictors of hysterectomy prevalence among women in the United States. Am J Obstet Gynecol. 2022 Oct;227(4):611.e1-611.e12.
Elgi MC, Viswanath L. Knowledge of Women on Hysterectomy. J South Asian Feder Menopause Soc 2019; 7 (2):82-85.
RANZCOG, Clinical Guidance Statement: C-Gyn 25 Managing the adnexa at the time of hysterectomy for benign gynaecological disease [Updated: Feb 2023].
BPAC: Menopausal hormone therapy: where are we now? 2019
ANZJOG, Toward ‘net zero’ hysterectomy for Australia; New Zealand is already heading there… ANZJOG Feb 2022; 62 (1): 9-11.
Ovarian Cancer New Zealand Foundation, About Ovarian Cancer, [Updated: 16 Jan 2024].
Vikstedt, T., Arffman, M., Heliövaara-Peippo, S. et al. Change in medical practice over time? A register based study of regional trends in hysterectomy in Finland in 2001–2018. BMC Women’s Health 21, 242 (2021).
Baffour Awuah, G., Schauberger, G., Klug, S.J. et al. An age-period-cohort analysis of hysterectomy incidence trends in Germany from 2005 to 2019. Sci Rep 14, 15110 (2024).
[Updated: 14 July 2025]
